


AI in Physician Performance and Productivity Monitoring: The Future
An optimistic view with some worst case scenarios

An Optimistic View of AI in Physician Productivity and Performance
In previous weeks we’ve looked at how productivity and performance are measured in medicine and other industries. Today we’ll focus on the best case scenarios for currently available AI technology as applied to physician productivity and performance.
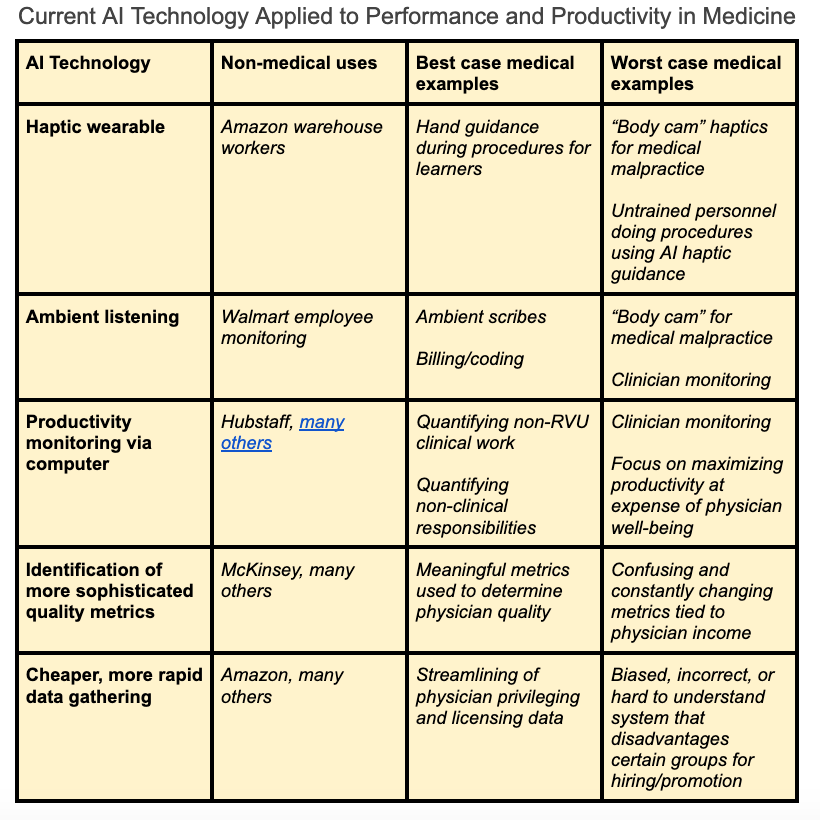
I don’t want to discount the very real worst case scenarios, some of which I’ve listed in the table below. The reality is that there are so many possible worst case uses of this technology that it would be overwhelming to attempt to list even the majority of them. I’m hopeful that AI will be an overall benefit in productivity and performance, though the engagement of physicians in these conversations is crucial. I’ve listed some opportunities below, along with the barriers and my guess at a timeframe.
Opportunities for AI impact
Physician Recruitment
Hiring decisions are one area that I’ve always been surprised hasn’t moved forward with technology. We still hire doctors based on…well, if they seem nice and know someone you know. In an age where there’s an exploding amount of public information about doctors available, there's a huge opportunity to use that data to find a good fit for a specific hospital or geographic area.
Physician Job Search
Not only does it make sense for hospitals to use data to recruit doctors; it also makes sense for physicians to use their data as part of their CV. They could have a “Clinical Quality Card” to present to potential employers to show that they do good work. Currently the main barrier is that
physicians usually don’t have access to their own outcome data. The health system collects and analyzes physician quality data, and CMS data often isn’t great quality and doesn’t capture huge swaths of patients like 23h obs, for example.
Barriers: Much physician data stored within health systems; unclear if physicians would pay for this service
Possible timeframe: 5-10 years
Physician Credentialing
A related aspect of recruitment is the burdensome licensing and credentialing process. AI should be able to find and verify almost all the relevant information quickly. A few companies are already doing this, but it should be commonplace
Barriers: Motivated payors
Possible timeframe: 2-5 years
Personalized Clinical Feedback
There are huge opportunities in personalized feedback for trainees and practicing physicians, as described last week.
Barriers: Cost, legality
Timeframe: Now-5 years
Clinical Documentation Burden
Many millions of dollars are flowing into this area, including from Amazon and Microsoft, mostly driven by LLMs that listen in to conversations and format the information into a note template. Emerging evidence seems encouraging with regards to improved efficiency and job satisfaction. Beyond just transcription, there's an opportunity to identify workflow inefficiencies and improve care coordination. Additionally, providing physicians with a concrete measurement of charting efficiency may help them get personalized recommendations for time-saving charting techniques.
Barriers: Cost of implementation and ongoing use
Possible timeframe: Now to 3 years
Non-clinical Administrative Burden
Administrative burden, particularly for academic and employed physicians who spend a large portion of their time on non-clinical tasks like meetings and emails, has always been difficult to quantify. As a result, nonsensical time allocations for non-clinical time are common. My personal favorite is the 0.05FTE allocation for a project. If you have gotten a project accomplished with a half day every other week, I applaud you. Much more common is either doing more than your allocated FTE - unpaid - or basically nothing other than occasionally showing up for a meeting.
People doing a lot of this work may actually benefit from having their time monitored (with consent, of course). Realizing how much time they’re actually spending on a project can help them realign priorities and ask for the appropriate amount of compensation to reflect the time spent. I know a lot of institutions like Stanford have tried giving non-monetary benefits for non-clinical work like dry-cleaning and babysitting. Maybe that’s a nice tax work-around, but in the future perhaps we can just see how long non-clinical assignments take and just…pay people for them. Female physicians do a disproportionate amount of non-clinical work that doesn’t progress their careers, and being able to demonstrate more accurately the demands of these lower-status positions will at least get them the compensation they deserve.
Barriers: Expense of monitoring systems, policies to discourage worst-case behavior
Timeframe: Possibly this year if health systems are motivated to align payment with actual non-clinical time, likely much longer.
Quality Metric Development
Many of the quality metrics physicians are measured on are too narrow to be useful, so routine that they don’t improve practice, or reward charting more than actual patient care. In other fields like manufacturing, AI has helped improve data quality and develop metrics that actually help improve the end goal.
Barriers: Cost, motivation from the systems paying for the technology
Timeframe: 3-7 years
How do you hope AI will affect your productivity and performance? What worst-case scenarios are you concerned about?
If you’re a physician, join us at the ML for MDs Slack group, where we share resources and knowledge about the intersection of AI in healthcare.