

The reality gap between health tech and clinical practice
The reality gap between health tech and clinical practice
My patients aren't getting the memo about the health tech revolution

In the late 1800s, leaders of industry described the common knowledge about their fields:
The creator of the telegraph industry determined that “electric light will never take the place of gas”.
The scientist who developed the law of conservation of energy said “Radio has no future and X-rays will prove to be a hoax”
The list of “common knowledge” statements made by experts that turned out to be incredibly wrong is long: a World War II general said the invention of machine gun wouldn’t change warfare, the head of Warner Studios said that no one would want to hear actors talk, and a leading economist said stocks would never go higher in 1929.
These experts had made a series of assumptions that led to perceived and actual reality being so far apart that they were entirely wrong about what the future might hold.
Reading about health tech often gives me a similar feeling: perceived and actual reality are very far apart. As a field, we’ve bought into assumptions without examining the counter-arguments. These differences are especially apparent to me when I read about and discuss health tech then go directly to the hospital. The gap between what health tech describes and what my patients and colleagues say and do are often very far apart.
Viva la revolucion?
I was recently scrolling through LinkedIn and saw 7 posts in a row to the effect of “we are going to revolutionize healthcare with our app”. If you look at the Y Combinator list of health tech companies, it’s hard to find one without a synonym for “revolutionize” in its pitch. (Which, of course, makes sense if you’re asking for millions of dollars!)
Health tech taking over the field often seems like reality for someone like me who often hears health tech pitches, in which I am truly convinced of a team’s ability to solve a real problem in healthcare. However, in my role as a physician, I can tell you off the top of my head which apps my patients have mentioned using: Activity trackers, GoodRx, meditation apps. My experience fits with a study that asked people what health apps they use, where the pie chart shows large chunks related to wellbeing/stress reduction, and activity trackers, and tiny slivers for telemedicine and disease management.

How many people actually use health tech?
A big question is what “counts” as health tech: 93% of Americans use search engines to answer medical questions, and about a third use wearable technology. I don’t consider either of these part of the ‘health tech’ ecosystem, at least until the searches produce reliable information or wearables produce usable data.

Even when you include fitness trackers as health apps, half of the people who download them only use them for a few months.
Blame the patient
There’s an old saying in the OR: The surgeon blames the anesthesiologist, the anesthesiologist blames the surgeon, and they both blame the patient. Meaning that when something isn’t working, the medical system tends to assume it’s something inherently wrong with the patient: maybe they have an undiagnosed bleeding disorder and that’s why they keep bleeding, for example. Or maybe their untreated hypertension is causing hemodynamic instability.
Much of the health tech literature seems to combine this unhelpful approach with medicine’s old standby, paternalism. I found many articles with implicit messages like “the reason there’s not more uptake of healthtech is that old people and rural customers don’t know how to use their phones” and “marginalized groups don’t engage with the healthcare ecosystem”. These articles ignore the evidence that many people from marginalized groups actually posted more than others on social media during COVID, for example, or that many of my rural patients are quite savvy about telehealth appointments because their alternative is to drive 7 hours roundtrip to a major city.
Blame the healthcare workers and hospitals
The other frequent recipient of blame for lack of health tech adoption is hospitals and the people actually taking care of patients. Don’t get me wrong - there is plenty wrong with how hospitals and physicians have approached technological change in the past. But there’s an overarching sentiment of “hospitals and clinicians don’t know how to adapt to the present/future, which is why health tech hasn’t been more successful.” As this quote from a recent Harvard Business review article points out, hospitals actually adapt and change on a regular basis:
“Although the industry may seem stodgy and set in its ways, health care providers have had to transform themselves with some regularity, and they’ve shifted to deal with changes in reimbursement, the need to adopt electronic health records, the Covid-19 pandemic, and the need to expand beyond medical care to address social determinants of health (access to food, healthy environments, public safety). They could be better at transforming themselves, but they are not new to the challenge.”
This quote doesn’t even mention clinical changes with evolving guidelines and new studies, which is a fundamental part of healthcare that requires a huge amount of time and effort to do well. The idea that physicians and nurses refuse to change or don’t want to change is often (not always!) a way for healthtech companies to pass off blame for a solution for which there’s not a huge need. Nurses and physicians deserve more acknowledgement as innovators and instigators of change. Clinicians do a huge amount of change management, but somehow we’ve gotten labeled as impediments to progress.
A 2019 article by Neil Khosla notes that health systems run on an incredibly tight margin of around 1.7%, which necessitates not just clinical innovation but new ideas for optimizing supply chain, employee costs, and balancing community benefit. As the article points out, that small margin for error makes hospitals risk-averse because even investments that are small relative to their revenue may be huge relative to their operating profit.
Creating change without being able to change behavior
The supposed roles are well-established: physicians want to spend more money on patient care (of which they are sometimes but not always beneficiaries), insurers want to spend less money on patient care (of which they are always beneficiaries), and hospitals want to make more money (often to benefit their communities). The unusual aspect of healthcare is that none of these parties can effectively influence the others’ behavior. Insurers can’t force doctors to spend less on patient care, but doctors can’t make insurers pay for desperately needed services if they refuse, either. Health systems try to develop incentives for physicians to get them to provide more cost-effective care, but their tools are almost non-existent.
People actually want to be treated by…people
A recent Accenture survey on digital health found that communication, emotional support, and care coordination were the three most important reasons a patient chose a provider:
“When asked which factors were most important to creating a positive experience with a healthcare provider, people ranked “a medical provider who explains the patient’s condition and treatment clearly” (55%) as the most important factor with “a provider who listens, understands patient’s needs and provides emotional support” (52%) as a close second. The third-highest-rated aspect of a positive experience is well-coordinated communications and organization”
This may be the aspect that healthtech companies are most likely to forget. People might like a quick and easy experience for issues they think are not serious, like a cold or ear infection. But if they’re really worried about something, they want to talk to someone they trust. It’s really hard to build that kind of relationship completely on a platform. Patients are also very sensitive to the reputation of a physician and the health system; I often have patients tell me how much they’ve researched a certain doctor before getting a knee replacement or cancer treatment. Many see more than one doctor before deciding on treatment and often make their decision based on some combination of reputation and personal connection. Both of those factors - trusted recommendations and an emotional connection - are hard to develop with many health tech platforms.
Are we all guilty of overlooking reality?
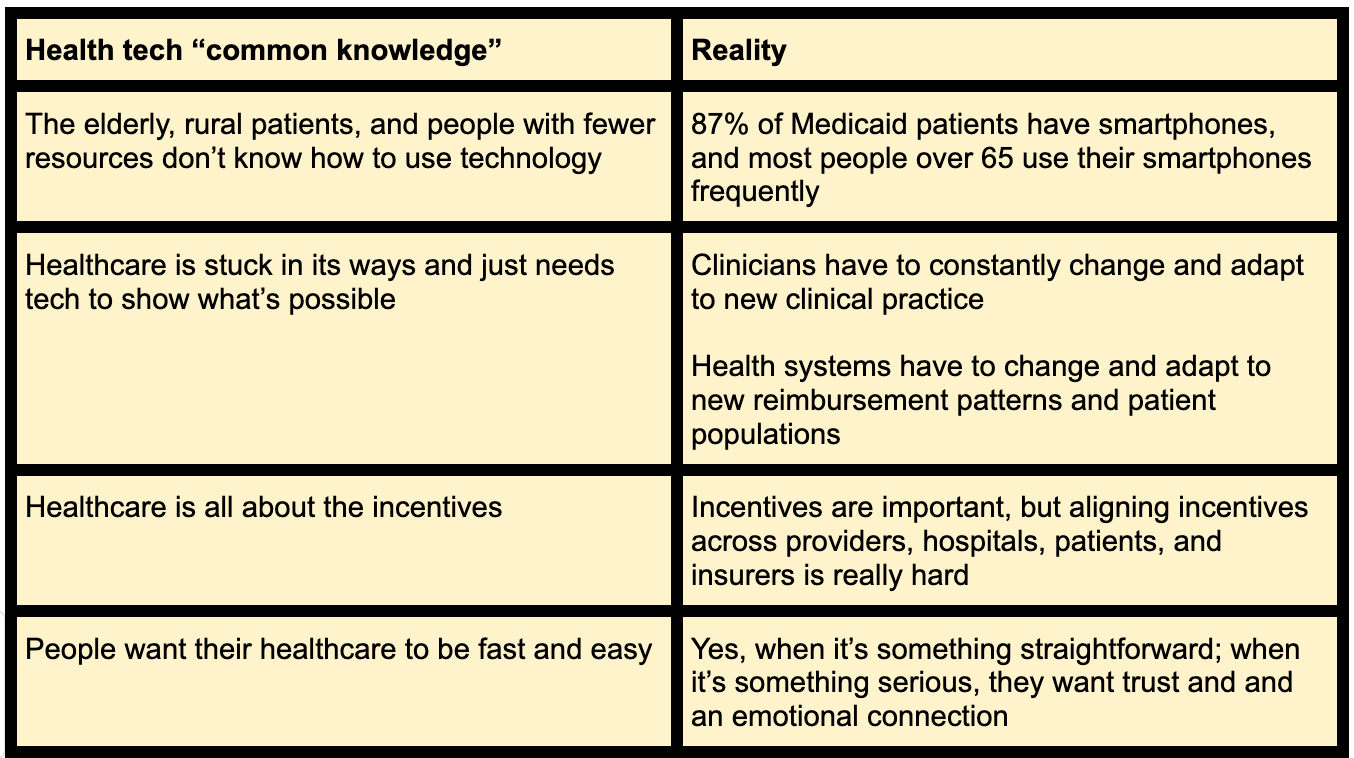
Yes, when it’s something straightforward; when it’s something serious, they want trust and and an emotional connection
Recently I’ve felt like we’re all walking around like the experts from early days of radio, movies, and electricity. We assume that we know what the main issues and best next steps are. But we don’t always take the time to go just a little deeper to question our underlying assumptions about how the future might unfold. There have been dedicated clinicians and administrators trying to make patients’ lives better for centuries, and patients are smart and tech savvy. If we started from these assumptions instead, would we decrease the gap between perceived and actual reality?